
Virtual Reality Training for Doctors Made Real by Columbia’s Clinical Innovation Lab
Have you ever thought, if only I had a [insert imaginary tool] I’d be better at [insert real task]? The folks at the Columbia Clinical Innovation Lab hear you. They believe the best way to advance medicine and patient care is to nurture ideas from people who work in the field and help turn those ideas into real products.
“Many new products are interesting but not useful in real-world clinical settings,” says Shunichi Homma, MD, chief medical officer of ColumbiaDoctors and the Margaret Milliken Hatch Professor of Medicine at Columbia University Vagelos College of Physicians and Surgeons.“We want to invent things people in medicine actually need.”
To encourage that innovation, the Clinical Innovation Lab was established nearly two years ago by Homma and Timothy Crimmins, MD, chief medical information officer at ColumbiaDoctors and associate professor of medicine at Columbia University Vagelos College of Physicians and Surgeons.
Project: virtual reality training for ultrasound-guided central line placement

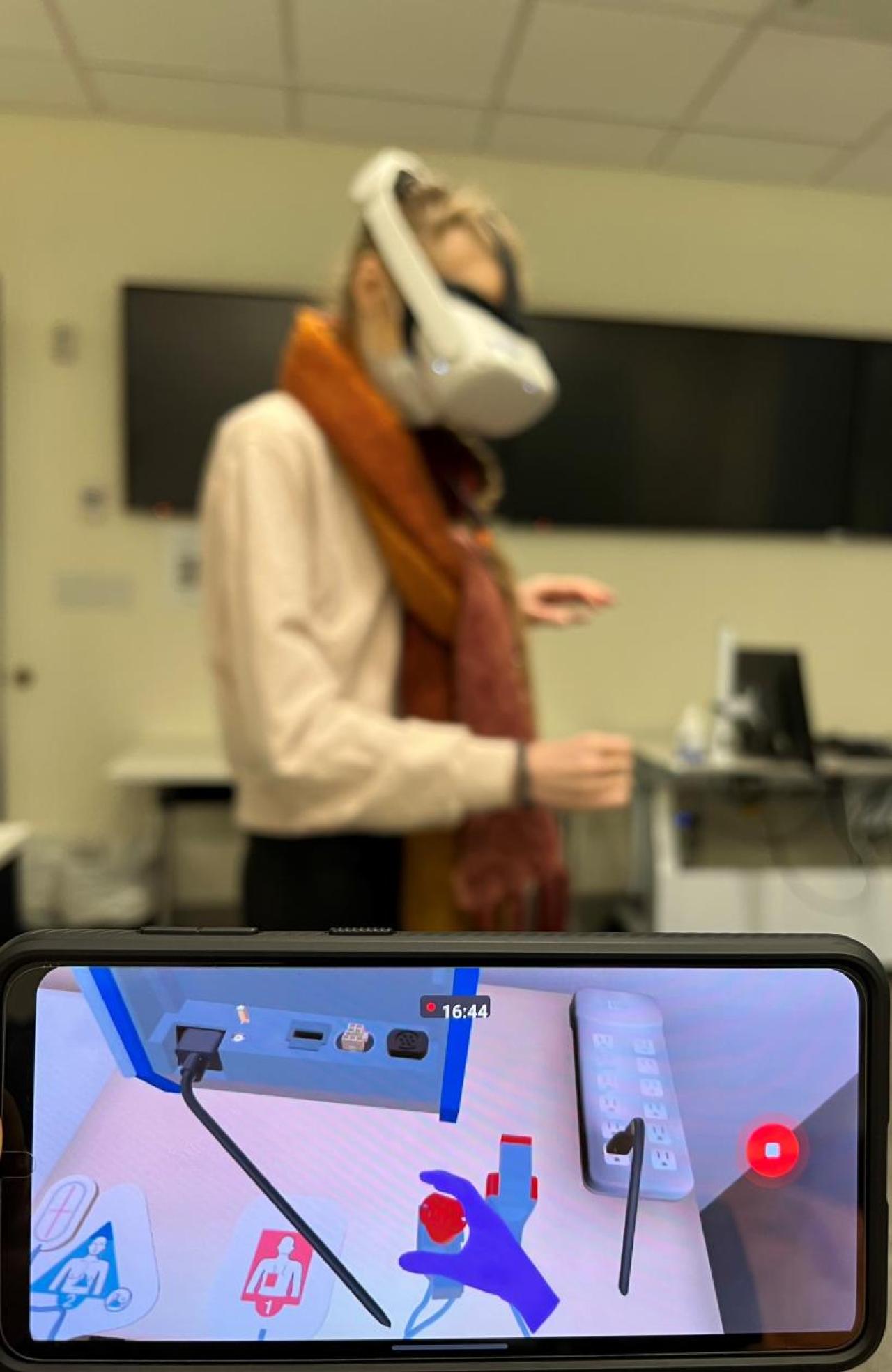
Medical training via virtual reality. Students honing their skills in placing a central line using a virtual reality trainer developed by Columbia physicians and researchers. The project receives funding from the Clinical Innovation Lab at ColumbiaDoctors. Photo: Robert Maniker/Columbia University Irving Medical Center.
Columbia anesthesiologist Robert Maniker, MD, is part of a team that received seed funding from the lab.
Maniker is always thinking about ways to improve medical education and previously contributed to creation of the Anesthesia Toolbox, an online learning resource used by almost every anesthesia program in the country. But sometimes hands-on practice is necessary to master hand-eye coordination for delicate and complex procedures, like central line placement. He asked himself how training could be standardized for such procedures to help medical students and professionals everywhere become competent and confident.
His answer: virtual reality.

“Web-based learning tools are great because they’re widely disseminated. But they’re not interactive. A simulation center is immersive and safe: You can practice as much as you need, and you can’t injure anyone. But faculty time is limited and everything about simulation is expensive,” Maniker says.
The use of specialized plastic mannequins for training and the staff needed to run a simulation center cost millions of dollars, so such training is not accessible to all health care workers. Making simulation available—through virtual reality—to more medical students, residents, and staff became a focus.
“Long story short, VR has the capacity to reach a bigger audience,” Maniker says.
Maniker has been working with another virtual reality enthusiast, David Kessler, MD, associate professor of emergency medicine, and Columbia professor of computer science Steven Feiner, PhD, to create simulated ultrasound training programs: how to’s in virtual reality. To the Innovation Lab’s board they proposed Virtual Reality Training for Ultrasound-Guided Central Line Placement, an extension of their simulation work in progress.
Feiner is director of Columbia University’s Computer Graphics and User Interfaces Lab, where augmented and virtual reality (AR and VR) are researched and developed. Kessler, also interested in training and innovation, is the ideal collaborator. The doctors combined efforts and met regularly with Feiner and his team of students to develop their medical training ideas.
Over time, in Feiner’s lab, a VR ultrasound trainer was built. Just put on a headset, pick up an ultrasound transducer (probe), and learn to scan and insert the central line into a virtual patient in front of you.
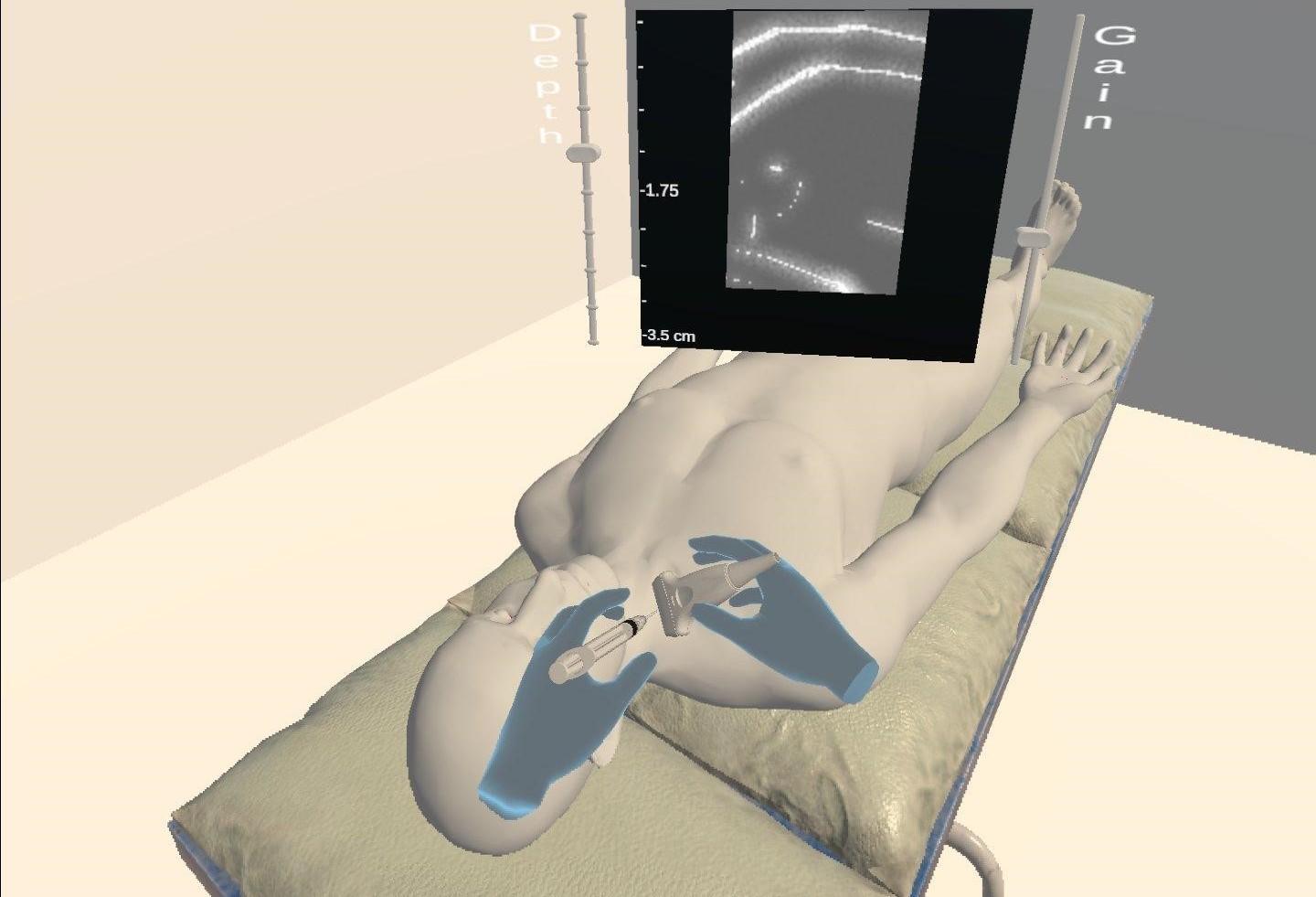
Virtual Central Line Placement. With a virtual reality system developed by Columbia researchers, trainees can put on a VR headset, pick up an ultrasound probe, and learn to insert a central line. Central lines provide patients with more medications, fluid, or blood when an IV is too narrow. To insert it properly, doctors use ultrasound to guide a needle into the correct vein. It takes finesse and extraordinary hand-eye coordination. With virtual reality, such medical training can reach a wider audience of learners who don't have access to expensive simulation centers. Image: Robert Maniker/Columbia University Irving Medical Center.
Simple to use but not easy to create. It took a team of coders, computer scientists, designers, engineers, physicians, and researchers about a year to create the VR ultrasound scanner. The team is now working to create the step-by-step training module.
And it’s only a starting point. The team is looking to expand their VR training system to other ultrasound-guided procedures, like ultrasound-guided nerve blocks used to manage pain. “So many procedures that we do now in medicine are ultrasound guided,” says Maniker.
Maniker sees a big future for VR in medical training: “We can create entire training curricula around VR. There’s no doubt that in 10 or 20 years the vast majority of simulation will be done in a virtual world, not the archaic live plastic world.”
Attracting investors
Winning the grant from the Innovation Lab helps the VR medical development team solve one challenge with product development: time. “You can conceptualize something, but you can’t create it in a day,” says Maniker. During the life of the project, student assistants graduate, and others start fresh. For greater consistency, they’ve used the Lab’s grant money to hire a new software developer, the first team member not connected to the University.
Next year, the team will work with five departments at the medical center to pilot the prototype.
Once it’s viable, the product goes to the Innovation Lab for review and analysis. Does it work? Is it helpful? If so, the lab will show it to investors who can complete the build.
“We want to move as rapidly as possible to evaluate feasible ideas, then take them to investors,” says Corinne DePue, the lab’s director of organizational development and transformation. “If we're going to fail, let's fail fast and move to the next project. And if we succeed, let's move as quickly as we can to develop products everyone in clinical medicine can truly use.”
The Innovation Lab is currently supporting five projects, including Maniker’s.
“Interdisciplinary collaboration is the best way to advance medicine," says Homma. “And Columbia’s Clinical Innovation Lab is the hub where we can capitalize on the University’s intellectual prowess to make a difference for our patients.”
| Request for Proposals. The Innovation Lab seeks people in health care who have an idea—within the framework of patient care—but don’t know where to start. They’re also seeking anyone with expertise in developing products that advance clinical medicine. Submit your idea. |
References
Shunichi Homma, MD, is the Margaret Milliken Hatch Professor of Medicine, deputy chief of the Division of Cardiology, and director of noninvasive cardiac imaging at Columbia University Vagelos College of Physicians and Surgeons. He also is the chief medical officer at ColumbiaDoctors.
Timothy Crimmins, MD, is associate professor of medicine and medical director of the Non-Invasive Vascular Medicine Lab at Columbia University Vagelos College of Physicians and Surgeons.
Robert Maniker, MD, MSc, is associate professor of anesthesiology and director of the Acute Pain Service at Columbia University Vagelos College of Physicians and Surgeons.
Steven K. Feiner, PhD, is professor of computer science and director of the Computer Graphics and User Interfaces Lab at Columbia University.
David Kessler, MD, MSc, is associate professor of pediatrics (in emergency medicine) at Columbia University Vagelos College of Physicians and Surgeons.
Columbia Clinical Innovation Lab