Newer Gene Therapies, Tested at Columbia, Could Give Sickle Cell Patients More Options
Results from clinical trials of two experimental gene therapies for sickle cell disease—conducted at Columbia University Irving Medical Center and other centers—show that new gene-editing techniques free patients from frequent painful episodes caused by their misshapen blood cells and could give patients more treatment options.
Results from trials of the two therapies—reni-cell from Editas and risto-cel from Beam Therapeutics—were published earlier this year in the New England Journal of Medicine.
“These therapies, and the two gene therapies already approved for sickle cell, have been generally life-changing for our patients, and the outcomes have been phenomenal,” says Markus Mapara, professor of medicine at Columbia University Vagelos College of Physicians and Surgeons and director of the Blood and Marrow Transplantation/Cell Therapy Program at NewYork Presbyterian Hospital/Columbia University Irving Medical Center.
Though the company that tested reni-cel is no longer developing the therapy, Beam Therapeutics is planning to apply for FDA approval of risto-cel later this year. “If it’s approved, risto-cel could give more patients an opportunity to be treated with gene therapy,” says Mapara, a co-author of the two studies who has led all adult trials for sickle cell gene therapies at CUIMC.
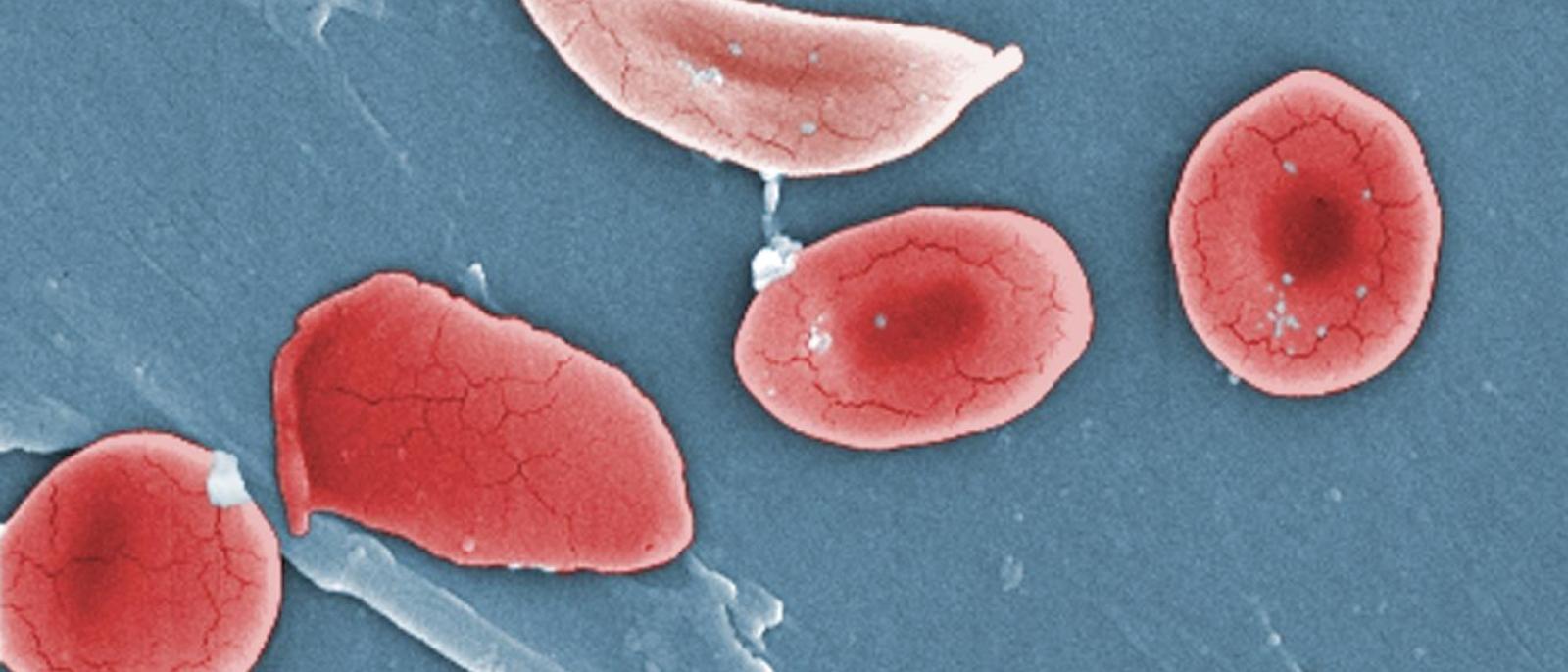
In sickle cell disease, a small mutation in a hemoglobin gene causes red blood cells to warp into crescent or sickle shapes. The sickled cells stick together into clumps that often block small blood vessels, starving tissues of oxygen.
The blockages also trigger severe “pain crises” that can last for days, disrupting school, work, and life, and frequently require hospitalization. Because these blockages lead to widespread organ damage over time, median life expectancy among sickle cell patients is only in the mid-40s. “Patients live in constant fear of the next pain crisis,” Mapara says.
Gene therapies edit the DNA inside a patient’s blood-producing stem cells to reduce sickling. “With these treatments, patients are essentially given a normal life; pain episodes disappear for the most part and frequent visits to the emergency department are eliminated,” he adds. “As more time goes by, the hope is that we’ll see less organ damage and patients will live longer.”
We spoke with Mapara about the new findings and remaining challenges for the field.
What’s different about these two experimental treatments from the gene therapies now available for sickle cell?
Both experimental therapies take a new approach to gene therapy for sickle cell than we’ve seen before. They both edit a stretch of DNA just in front of the fetal hemoglobin gene, and that turns the gene on. There’s good reason to turn on the fetal hemoglobin gene in sickle cells patients: We know patients who naturally produce higher levels of fetal hemoglobin, which is normally turned off after birth, have fewer sickled cells and their disease is less severe.
The clinical trials showed that this new approach was very effective in patients and is probably here to stay. (Casgevy, one of two currently approved gene therapies, also turns on fetal hemoglobin, but through a different, more indirect edit. Lyfgenia, the other FDA-approved gene therapy, inserts a complete hemoglobin gene into a patient’s blood-producing stem cells.)
The trial of risto-cel from Beam Therapeutics is, I think, groundbreaking from a number of aspects. Rather than using a CRISPR-CAS editing approach, risto-cel is created with base editing, which is highly efficient and leads to less DNA damage during the editing process.
Clinically with risto-cel, we saw a very high fetal hemoglobin level—an average of 60%—the highest level we’ve seen with gene therapy. That’s exciting because when the percentage of mutant hemoglobin drops to 30% or less, which we see in people who carry just one sickle cell gene, no sickled cells are produced.
It also seems that the whole editing procedure is somewhat softer on the stem cells, because they engraft more quickly when introduced back into a patient. That shortens the patient’s hospital stay, which can have a real, meaningful impact on quality of life, as well as reducing cost.
Why has Columbia been so involved in these trials?
Before gene therapy arrived, the only way to cure sickle cell disease was with a stem cell transplant using stem cells from a donor. Columbia has a very robust stem cell transplant program here for both adults and children with sickle cell disease.
The best outcomes with donor cell transplants are achieved in patients who have a matched donor, which is only the case in less than 20% patients. Half-matched donor transplants are also very promising but are associated with more potential toxicities. That’s why gene therapy is so attractive as it uses the patient’s own cells.
We’re one of the few centers in the world that has participated in clinical trials for all four therapies that have been tested to date.
We are one of the most experienced centers in the world at this point, with almost a decade of experience using gene therapies to treat patients with sickle cell and a similar condition called beta thalassemia.
Are there still improvements to be made with gene therapies for sickle cell?
The biggest challenge we face is that all these therapies rely on high-dose chemotherapy to eliminate old stem cells and make room for the modified stem cells. Patients are very vulnerable at this stage and must be kept in the hospital for weeks to prevent infections and manage the side effects of the high dose chemotherapy. When you look at the overall procedure, almost all major complications are driven by the need for this high-dose, conditioning chemotherapy. Eliminating it is one of the most important objectives for the field.
At CUIMC, we’ve started a trial to replace conditioning chemotherapy with a milder approach that uses an antibody to selectively deliver radiation to the bone marrow and other organs of the immune system (e.g. lymph nodes and spleen). We’ve treated one patient who had a transplant from a matched sibling , and everything is working well. So, we think the same conditioning could potentially work in the context of gene therapy as well.
The next big thing on the horizon is in vivo gene therapy. That could really transform the field, because conditioning to make space for transplanted cells wouldn’t be required at all. With in vivo gene therapy, the gene editing happens inside the patient’s bone marrow, and we wouldn’t need to transplant cells. The preclinical studies look very promising, and we hope to offer these therapies to our patients through clinical trials once they’ve begun.
It is truly amazing how the field has changed over the last years. The introduction of these new gene therapies has already made a great impact on the life of the patients who participated in the trials. It’s even more gratifying that these therapies are now available as standard of care, and we will see many more patients with SCD benefitting. Further improving the current therapies and making them accessible for all patienst are the top goals for the next years.