Implanted Pump Safely Delivered Chemo Straight to the Brain in Patients with Brain Cancer
New study shows implantable pump safely and effectively bypasses the blood-brain barrier to deliver drugs to the brain
A significant obstacle to treating brain cancer is not the cancer, but the brain itself.
The blood-brain barrier is an important aspect of the brain’s blood vessels that prevents poisons, viruses, and bacteria in blood from infiltrating the brain—but it inadvertently blocks most therapeutic substances.
Nanoparticles, focused ultrasound, clever chemistry, and other innovative ideas are being tried to overcome the barrier and deliver treatments to the brain. Now, neurosurgeons at Columbia University and NewYork-Presbyterian are taking a more direct approach: a fully implantable pump that continuously delivers chemo through a tube inserted directly into the brain.
A new study, the first to test the implantable pump system in patients with brain cancer, shows that the novel approach effectively kills brain tumor cells and offers a safe way to treat patients with brain cancer. Results from the study, a phase 1 trial involving five patients with recurrent glioblastoma, were published in the November issue of Lancet Oncology.
“This new approach has the potential to transform treatment for patients with brain cancer, where the outlook for survival remains very poor, though more testing is needed in patients with earlier-stage tumors and with different types of chemotherapy,” says Jeffrey Bruce, MD, the Edgar M. Housepian Professor of Neurological Surgery Research at Columbia University Vagelos College of Physicians and Surgeons, a neurosurgeon at NewYork-Presbyterian/Columbia University Irving Medical Center, and a senior author of the study.
Brain cancer is resistant to treatment
Patients with brain cancer are first treated with surgery to remove as much tumor as possible, followed by radiation and chemotherapy.
In theory, doctors could give patients higher doses of chemotherapy—via pills or intravenously—to overcome the blood-brain barrier and get more chemo into the brain. But at higher doses, the medications cause too many side effects in other parts of the body, and patients cannot tolerate them.
As a result, the amount of chemotherapy that can be given safely to patients with brain tumors is invariably ineffective.
"The tumors inevitably grow back,” says Bruce, who is also director of the Bartoli Brain Tumor Research Laboratory at Columbia University Vagelos College of Physicians and Surgeons. “And when they grow back, there's no proven treatment for them.”
Median survival for patients who undergo treatment for glioblastoma is just over 12 months. Once patients’ tumors return, their prognosis is usually only around four or five months.
New system breaches the brain’s barrier
Over the last decade, Bruce and his team have been working on a pressurized pump to bypass the blood-brain barrier and direct chemotherapy to the area of the brain where the tumor is located.
But early prototypes, which included an external pump attached to a catheter inserted through the skull, allowed only a single treatment limited to a few days before running the risk of infection. Patients also had to remain in the hospital while hooked up to the pump.
To overcome this limitation, Bruce’s team designed a new prototype that has no external parts and can be left in place for as long as needed. A small pump is surgically implanted into the abdomen and connected to a thin, flexible catheter threaded under the skin. Stereotactic imaging guides the surgical placement of a catheter precisely in the area of the brain where the tumor and any residual cancer cells are located.
“If you pump in the drug very slowly, literally at several drops an hour, it penetrates into the brain tissue,” says Bruce, who first tested the method extensively in animal models. "The drug concentration that ends up in the brain is 1,000-fold greater than anything you are likely to get with intravenous or oral delivery.”
Similar implantable pumps are available to deliver pain medication to the spinal cord and can remain in place for years. The pump can be refilled or emptied with a needle. Wireless technology is used to turn the pump on and off and control the flow rate, ensuring that the medicine seeps in slowly and saturates the tumor without leaking out around the catheter.
“Most drugs would be more effective if you could give them on a long-term basis without side effects,” Bruce says. “The pump can stay in place for a long period of time, so we can give higher doses of chemotherapy directly to the brain without causing the side effects that we get with oral or intravenous chemotherapy.”
Study demonstrates safety and feasibility of implantable pump
In the new study, the pumps were implanted in patients with recurrent glioblastoma and filled with topotecan, a chemotherapy drug used to treat lung cancer, and gadolinium, a tracing agent to track distribution of the drug. (Previous studies in Bruce’s lab suggested that local delivery of topotecan, which targets actively dividing cells, may be more effective than current therapies for glioblastoma.)
The patients had four treatments over the course of one month; each week, the pumps were turned on for two days and off for five days. Patients went about their normal routines at home while treatment continued, drip by drip.
"The patients were walking, talking, eating—doing all of their normal daily activities. They wouldn’t even know whether the pump was on or not,” Bruce says.
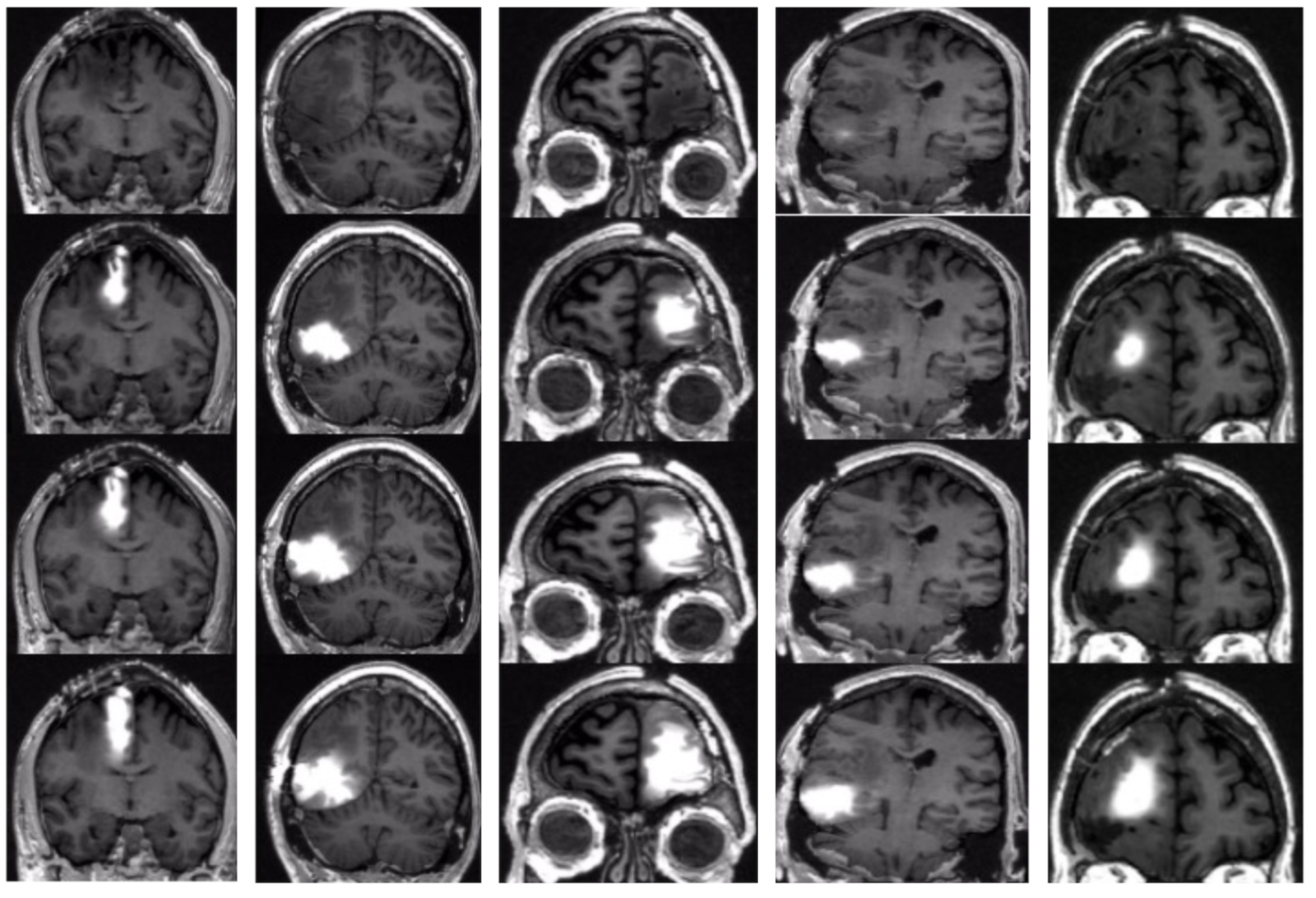
MRI scans show that chemotherapy delivered via the pump saturated the area in and around each patient's brain tumor. Top images show the brain before treatment; lower images were taken 14, 24, and 48 hours after treatment started. Image: Jeffrey Bruce, Columbia University Irving Medical Center.
None of the patients had serious neurological complications. And MRI scans showed that chemotherapy had saturated the area in and around the tumor.
Though the number of patients was too small to detect an overall survival benefit, a unique analysis of pre-treatment and post-treatment biopsies overseen by Peter Canoll, MD, PhD, professor of pathology & cell biology at Columbia, director of neuropathology at NewYork-Presbyterian/Columbia University Irving Medical Center, and a senior author of the study, showed that the chemotherapy was working: The number of actively dividing tumor cells decreased significantly, whereas normal brain cells were not affected.
Patient-focused approach to treating brain cancer
New studies are being planned to determine if the treatment is also safe for patients with newly diagnosed glioblastoma and if it can improve survival.
“A lot has already happened to make the tumor harder to treat by the time initial therapies fail, so we think that the pump will work even better with the newly diagnosed patients,” Bruce says. “This approach would give us the ability to change the treatment over time and consider using other types of chemotherapy that would not be effective if given systemically but may be much more effective when delivered directly to the brain.”
References
More information
The paper, titled “Chronic convection-enhanced delivery of topotecan for patients with recurrent glioblastoma: a first-in-patient, single-centre, single-arm, phase 1b trial,” was published in the November issue of Lancet Oncology.
Other authors (all from Columbia University and NewYork-Presbyterian unless otherwise noted) are Eleonora F Spinazzi, Michael G Argenziano, Pavan S Upadhyayul, Matei A Banu, Justin A Neira, Dominique M O Higgins, Peter B Wu (UCLA Geffen School of Medicine), Brianna Pereira, Aayushi Mahajan, Nelson Humala, Osama Al-Dalahmah, Wenting Zhao, Akshay V Save (NYU Grossman School of Medicine), Brian J A Gill, Deborah M Boyett, Tamara Marie, Julia L Furnari, Tejaswi D Sudhakar, Sylwia A Stopka (Brigham and Women’s Hospital, Harvard Medical School), Michael S Regan (Brigham and Women’s Hospital, Harvard Medical School), Vanessa Catania (Brigham and Women’s Hospital, Harvard Medical School), Laura Good, Stergios Zacharoulis, Meenu Behl, Petros Petridis, Sachin Jambawalikar, Akiva Mintz, Angela Lignelli, Nathalie Y R Agar (Dana-Farber Cancer Institute), Peter A Sims, Mary R Welch, Andrew B Lassman, Fabio M Iwamoto, Randy S D’Amico (Lenox Hill Hospital), and Jack Grinband.
The study was funded with grants from the National Institutes of Health (R01CA161404, R01NS103473, P30CA013696, 5P30CA013696-43, 5UG1CA189960-04, P41EB028741, UL1TR001873 and U54 CA210180), the William Rhodes and Louise Tilzer Rhodes Center for Glioblastoma, the Khatib Foundation, the Gary and Yael Fegel Foundation, and the Michael Weiner Glioblastoma Research Into Treatment Fund.
Author disclosures are included in the article.