
As Breast Cancer Awareness Month Ends, These Facts Are Worth Remembering
Breast cancer doesn’t take a break when November rolls around and the pink ribbons of October’s breast cancer awareness month fade from view.
Physicians at Columbia University Vagelos College of Physicians and Surgeons have been speaking and writing about what people, not just women, should know about breast cancer.
Here, we’ve summed up some of their latest advice, good for all 12 months of the year.
Know your risk
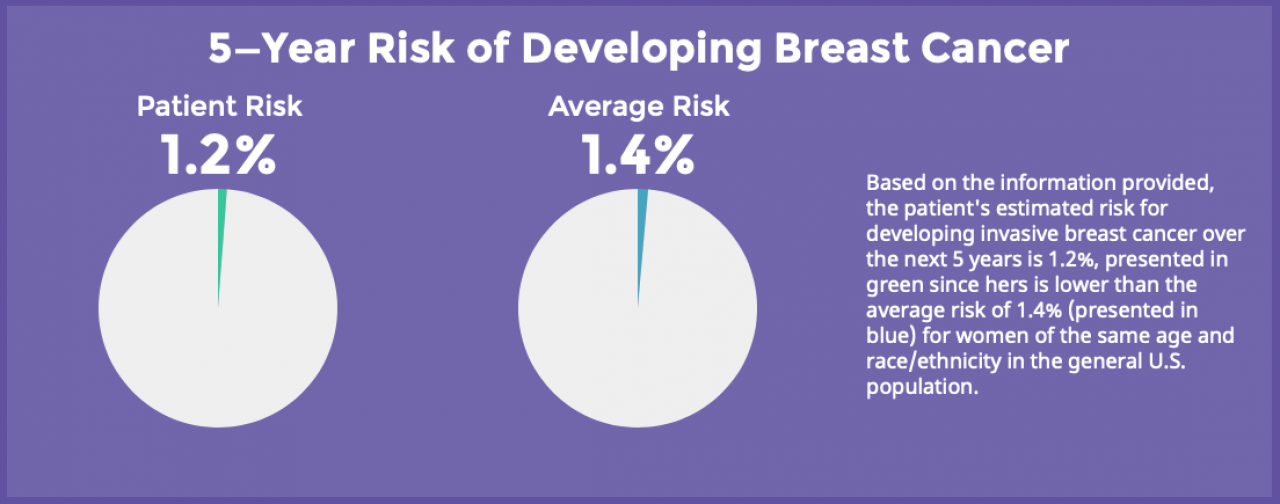
Knowing your risk status is the most important first step in mapping out a personalized screening program, say Columbia breast surgeon Luona Sun, MD. Image: example from the breast cancer risk assessement tool at the National Cancer Institute.
When breast cancer is caught early, the outcome is much better.
“Thanks to greater awareness and more advanced exams and screenings, breast cancer is caught at an earlier stage than ever before,” says Luona Sun, MD, assistant professor of surgery at Columbia University Vagelos College of Physicians and Surgeons and a breast surgeon at Columbia University Irving Medical Center/NewYork-Presbyterian.
“Knowing your risk status is the most important first step,” Sun says. This means having a consultation with your doctor to determine your risk. It could also include genetic testing—if the patient is comfortable with it and wants it—and a full family history evaluation.
Based on a person’s risk level and age, doctors can map out a personalized screening plan moving forward.
For people with average risk, the American Cancer Society recommends that women 45 to 54 years old should get annual mammograms, and women between 40 and 44 have the option to begin annual screening. [See the full recommendations here].
Practice breast self-awareness
Everyone should practice breast self-awareness, says Stacy Ugras, MD, assistant professor of surgery at Columbia University Vagelos College of Physicians and Surgeons and a breast surgical oncologist at NewYork-Presbyterian.
The simplest way to do that is by looking at your breasts in the mirror with arms both up and down, making sure the breasts are symmetric and that there are no inconsistencies between the two. If there is evidence of skin dimpling or redness, discharge, or scaling of the nipples, tell your doctor. Symptoms like these present physically on the skin’s surface and you can easily monitor them on your own.
As for performing a breast self-exam, “there’s no right or wrong way,” Ugras says. “Many times, patients become overwhelmed and believe they are doing it incorrectly, but I always encourage them to focus on the big picture.”
Some Black and Hispanic women have greater risk

Getty Images
“A report from the National Cancer Institute supported research showing that aggressive forms of breast cancers are common in younger African American/Black and Hispanic/Latina women living in low socioeconomic areas,” says Elise Desperito, MD, assistant professor of radiology at Columbia University Vagelos College of Physicians and Surgeons and chief of breast imaging at NewYork-Presbyterian.
These aggressive forms of breast cancer, such as triple negative breast cancer, are less responsive to standard cancer treatments and are associated with poorer survival.
“All women should be evaluated for breast cancer risk no later than age 30,” Desperito adds. “[but] breast cancer risk assessment at age 30 is particularly important for these women.”
Treatments are improving
Within just the past few years, at least four or five additional drugs have been approved for HER2-positive breast cancer.
“Although it is a more aggressive form of breast cancer, it is also a type of breast cancer that responds well and is very sensitive in general to chemotherapy and targeted therapy,” says Columbia oncologist Katherine Crew, MD, associate professor of medicine at Columbia University Vagelos College of Physicians and Surgeons.
“Even in patients who have metastatic disease, women are living longer—sometimes for more than five years—with advanced breast cancer.”
Clinical trials promise more advances
For patients who have all their lymph nodes removed during surgery, about 30% will develop lymphedema, a buildup of fluid in the arm that can be painful.
“We're starting to do more and more what we call axillary reverse mapping when we do lymph node dissections,” says Roshni Rao, MD, chief of breast surgery and the Vivian L. Milstein Associate Professor of Surgery at Columbia University Vagelos College of Physicians and Surgeons. “A study at Columbia, opened by Bret Taback, MD, as part of a national trial, is an effort to try to better visualize these tiny lymphatics so that more can be preserved at the time of surgery to potentially avoid lymphedema in the future.”
3D mammography gives women with dense breasts more options
“If you’re told you have dense breasts, definitely reach out to your doctor to discuss whether additional tests might be appropriate,” says Lauren Friedlander, MD, assistant professor of radiology at Columbia University Vagelos College of Physicians and Surgeons.
“The only way you know you have dense breasts is when a radiologist looks at your mammogram,” Friedlander adds. “Dense breasts are not something your doctor can detect on a physical examination or not something you yourself can feel.”
Having dense breasts does not mean you will get breast cancer. It does mean you need to be vigilant and get mammograms once a year.
“3D mammography does a bit better at finding breast cancers in all women but particularly in women with dense breast tissue,” Friedlander says.
Related News
A Voice for Cancer Patients
Desirée Walker is a native New Yorker who serves on the Herbert Irving Comprehensive Cancer Center’s Patient Advocacy Board. After receiving her first breast cancer diagnosis at age 38, Walker quickly threw herself into patient advocacy and has worked with organizations and agencies to address health care inequities.
“I recall public service announcements only saying that the incidence of breast cancer was high for Caucasian women,” she says in a recent HICCC interview.
“After my recovery, I began outreach in communities of African heritage to share my story. It was important to me to be a face of the disease and encourage my community to be informed about breast cancer.”
Karin's Story: Early Detection and New Radiation Therapy Made All the Difference
Columbia breast cancer patient Karin Diamond credits regular mammograms for catching her cancer early and her surgeon's use of intraoperative radiation for keeping her cancer-free. Read more in CUIMC News.
Rethinking Routine Mammography Among Older Women
Underutilization of breast cancer screening by some groups is a well-known problem, but mammography can also be overused. Columbia researchers are deploying “de-implementation science” to help improve outcomes and reduce unnecessary procedures.
Read more about the project on the Irving Institute for Clinical and Translational Research website.